
She thought it was just a cough: How ignorance fuels avoidable pain among tuberculosis patients
By Oluwaseyi Elizabeth Jimoh
When Mrs. Titilope Olarewaju (pseudonym) began coughing, it seemed like nothing more than a minor irritation. The Lagos-based mother of three was in her mid-forties—vibrant, hardworking, and devoted to her family. Between managing her career and running her household, she brushed off the lingering cough as a trivial inconvenience, something that would go away on its own.
But it didn’t.
Months later, she collapsed. Her sudden death left her family reeling, searching for answers. At first, there was no clear explanation for what had happened. It wasn’t until weeks later, when one of her children developed a persistent cough and was taken to the hospital, that the truth emerged: tuberculosis (TB).
Further investigation revealed a painful link—Mrs. Olarewaju had likely been living with undiagnosed TB for months, unknowingly spreading the infection to her child.
Her story is tragically common. Tuberculosis, an airborne disease, spreads through coughing or sneezing, often thriving in silence until it is too late.
NIGERIA’S HIDDEN TB BURDEN
According to the Global TB Report 2022, an estimated 2.9 million TB cases were missed globally. Nigeria ranks sixth in the world and first in Africa among countries with the highest burden of undetected cases.

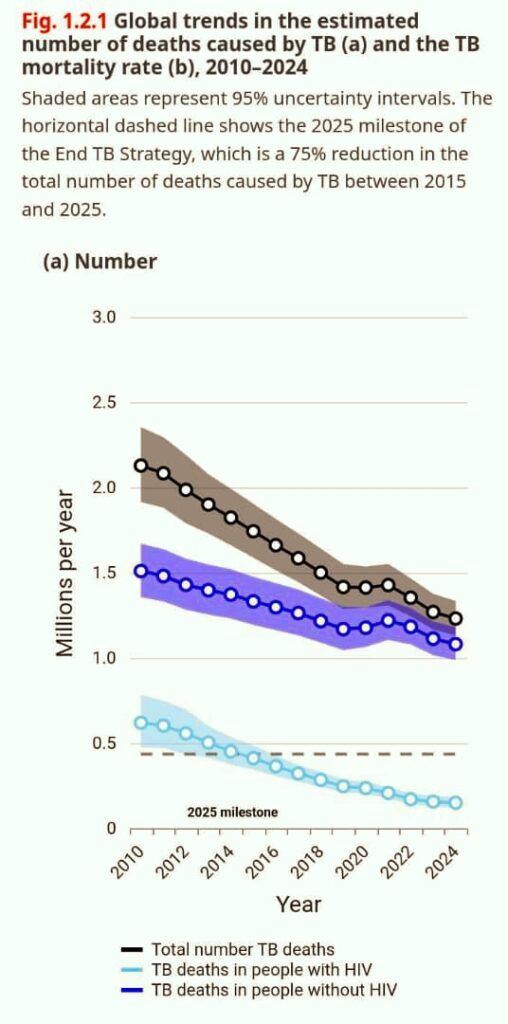
Tuberculosis remains one of the top ten causes of death worldwide, disproportionately affecting children under five and people living with HIV. The World Health Organization (WHO) reported that over 1.23 million people died from TB in 2021. While there has been a 29% reduction in TB deaths since 2015, the disease continues to devastate millions, with 10.7 million new cases recorded globally in 2024.
“MANY STILL THINK IT IS SPIRITUAL”
One of the biggest challenges in tackling TB in Nigeria is not just access to care, but a crippling lack of awareness.
“Many people see TB as a death sentence or a spiritual attack,” explains Dr. Olusola Sokoya, Coordinator of the Lagos State TB, Leprosy, and Buruli Ulcer Control Programme. He notes that less than 30% of Nigerians are aware of TB symptoms.
“While patients are often willing to disclose conditions like hypertension or diabetes, TB is different,” he adds. “There is fear, stigma, and misinformation. People hide it. This silence can be deadly.”
Dr. Sokoya emphasizes that TB is curable, contrary to widespread myths. “TB is not spiritual, hereditary, or generational. It is a bacterial infection caused by Mycobacterium tuberculosis and spreads through the air when an infected person coughs or sneezes.” Early diagnosis and strict adherence to treatment, he says, can save lives and prevent complications.
THE COST OF DELAY
Across Nigeria, similar stories of delayed care abound.
In Ondo West Local Government Area, a young man, Mr. Adedokun Titus, endured months of coughing and was repeatedly misdiagnosed with typhoid. Even after his eventual TB diagnosis, religious leaders advised him to prioritize spiritual intervention over medical care, framing his illness as a “spiritual attack.” By the time he began proper treatment, his condition had significantly worsened.
In Lagos, another survivor, Mr. Abdulsalam Abdulquadri, initially turned to herbal remedies before seeking hospital care. “I thought it was something spiritual,” he recalls. He was eventually diagnosed with drug-resistant TB, requiring an intense treatment regimen of over 20 pills a day and painful injections—an ordeal he describes as “almost unbearable.”
RISK FACTORS AND STRUCTURAL CHALLENGES
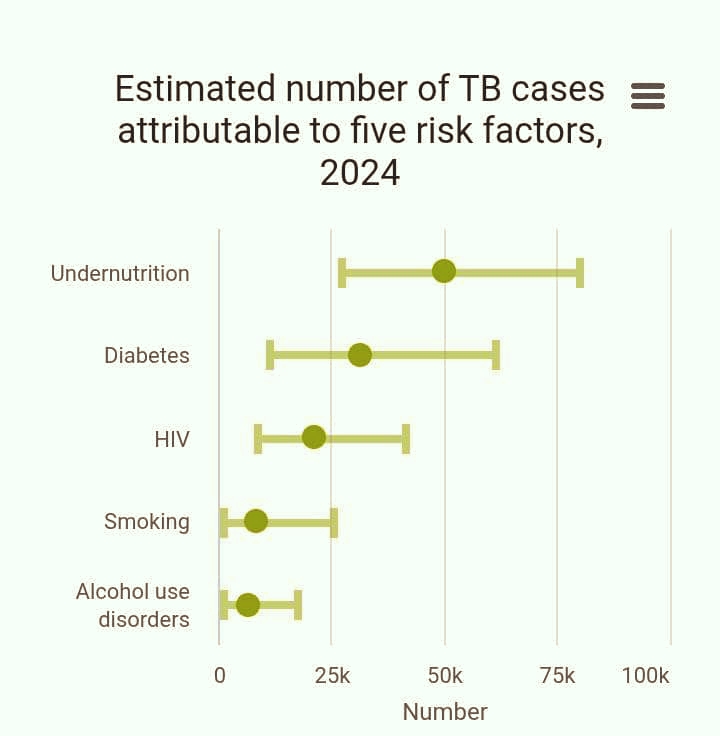
Tuberculosis thrives in environments shaped by inequality and limited resources. Key risk factors include:
- Poverty, which restricts access to healthcare.
- Malnutrition, which weakens the immune system.
- Poor sanitation and overcrowding, which facilitate transmission.
Even the wealthy are not immune, particularly when exposed to infected individuals in close living environments.
In Nigeria, the TB prevalence rate is estimated at 332 per 100,000 people, with an incidence rate of 219 per 100,000. Yet in Lagos, a city of nearly 30 million people, awareness of TB symptoms remains alarmingly low—at just 27%.
STIGMA, STRUGGLE, AND SURVIVAL
For many TB patients, the battle is not just medical—it’s social.
Mrs. Kadri Oluseyi, a TB survivor and HIV patient, initially dismissed her symptoms and turned to unconventional remedies. “I believed it was a spiritual attack,” she says.
Her condition deteriorated, and when she finally sought medical help, she faced stigma—not just from her community but sometimes from the healthcare system itself.
“I had to travel long distances to access treatment, and when I arrived late, I was turned away,” she recalls. At one point, overwhelmed and isolated, she stopped taking her medication altogether.

It was only after receiving compassionate care from a doctor who treated her with dignity that she began to recover. Now, she uses her experience to educate others.
“TB doesn’t respect anyone,” she says. “It doesn’t care if you’re educated, illiterate, rich, or poor.”
She emphasizes the importance of providing not just awareness but also practical support for patients. “Focusing on TB awareness is good, but nutritional support and economic empowerment are just as important,” she says.
BELIEFS, MYTHS, AND DELAYED CARE
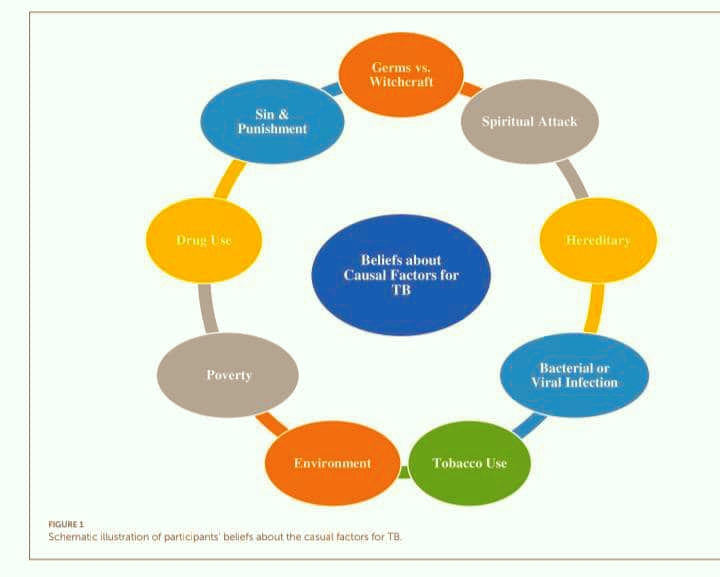
A 2024 study by Adeoye, Michael, and Agbana in Frontiers in Sociology examined TB patients in Oyo State who delayed seeking care. The findings revealed deeply rooted misconceptions:
- TB was often attributed to spiritual attacks or witchcraft.
- Some believed it was punishment for wrongdoing.
- Others linked it to hereditary causes or environmental exposure.
Local names for TB, such as “Ikofe” (dry cough) and “Iko jedojedo” (cough that consumes the liver), reflect these beliefs. Many respondents openly rejected scientific explanations, insisting that germs were not responsible for the disease.
MORE THAN MEDICINE
Even when patients seek care, challenges persist.
Elizabeth Moses, a woman in her fifties who underwent preventive TB treatment after exposure through a family member, describes the hidden burdens patients face.
“Treatment is free,” she says, “but everything else is not.” She highlights the increased hunger caused by medication, financial strain, and the difficulty of accessing care.
Survivors and experts alike agree: tackling TB requires more than awareness campaigns. It demands:
- Nutritional support for patients.
- Financial assistance for transportation to health facilities.
- Compassionate and stigma-free healthcare services.
- Community-based education tailored to cultural beliefs.
A COLLECTIVE RESPONSIBILITY
The WHO’s message is clear: “Yes! We can end TB.” But this vision can only become a reality if individuals, communities, and governments take action. - Educate yourself about TB symptoms and prevention.
- Seek testing early if symptoms appear.
- Adhere strictly to prescribed treatment.
- Reject myths and misinformation.
- Speak out against stigma and discrimination.
The tragedy of Mrs. Olarewaju and countless others highlights a painful truth: many TB-related deaths are preventable. Ignorance—whether rooted in misinformation, stigma, or systemic gaps—continues to cost lives.
Bridging this knowledge gap, strengthening healthcare systems, and fostering empathy in communities are essential steps toward ending tuberculosis. Because no one should die from a disease that is both preventable and curable.




Comments